胃栄養で順調に成長している子供に, 胃瘻挿入時に逆流防止手術を行うことを避ける[Choosing wisely]
今回は、小児の胃瘻挿入時に逆流防止手術に関してです。
この推奨を「choosing wisely」ではどのように記載されているのか紹介してみようと思います。

- Choosing wisely:小児の胃瘻挿入時に逆流防止手術
- 個々の症例で適応を考える
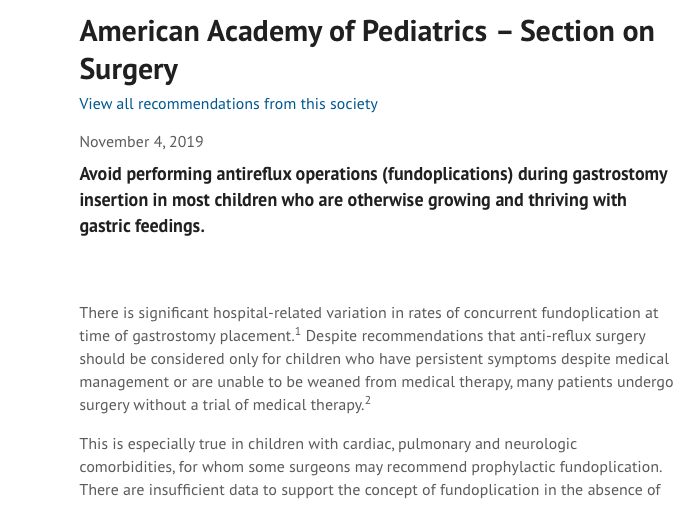
American Academy of PediatricsからのChoosing Wisely
胃栄養で順調に成長している子供に, 胃瘻挿入時に逆流防止手術を行うことを避ける[Choosing wisely]
Avoid performing antireflux operations (fundoplications) during gastrostomy insertion in most children who are otherwise growing and thriving with gastric feedings.
There is significant hospital-related variation in rates of concurrent fundoplication at time of gastrostomy placement. Despite recommendations that anti-reflux surgery should be considered only for children who have persistent symptoms despite medical management or are unable to be weaned from medical therapy, many patients undergo surgery without a trial of medical therapy.
This is especially true in children with cardiac, pulmonary and neurologic comorbidities, for whom some surgeons may recommend prophylactic fundoplication. There are insufficient data to support the concept of fundoplication in the absence of reflux, regardless of patient comorbidities. In fact, neurologically impaired patients are at higher risk for post-operative complications and/or fundoplication failure, and fundoplication does not lead to reduction in reflux-related admissions compared to gastrostomy alone. Definitive evidence supporting the effectiveness of fundoplication in children is lacking. Expert opinion-based guidelines state that fundoplication can be considered in infants and children with GERD who also meet any of the following criteria: 1) life threatening complications (e.g., cardiorespiratory failure) of GERD after failure of optimal medical treatment, 2) symptoms refractory to optimal therapy, 3) chronic conditions (i.e. neurologically impaired, cystic fibrosis) with a significant risk of GERD-related complications, 4) the need for chronic pharmacotherapy for control of signs and/or symptoms of GERD.
胃栄養で順調に成長しているほとんどの子供には, 胃瘻挿入時に逆流防止手術(fundoplication)を行うことは避けた方がよい。
逆流防止手術は、内科的治療にもかかわらず症状が持続している、あるいは内科的治療からの離脱が不可能な小児に対してのみ検討すべきであるという勧告にもかかわらず、多くの患者が内科的治療を試みることなく手術を受けている。
特に心疾患、肺疾患、神経疾患などの合併症を持つ子供たちには、予防的な腹腔鏡手術を勧める外科医もいるようだ。併存疾患の有無にかかわらず、逆流性疾患がない場合には逆流防止手術(fundoplication)を行うということを支持するデータは十分ではない。
実際、神経学的障害のある患者は、術後の合併症や逆流防止手術(fundoplication)の失敗のリスクが高く、逆流防止手術(fundoplication)は胃瘻造設のみの場合と比較して、逆流に関連した入院患者の減少にはつながらない。
専門家の意見に基づいたガイドラインでは、以下の基準のいずれかを満たす乳幼児や小児のGERDには逆流防止手術(fundoplication)を考慮してもよいとしている:
- 1最適な内科的治療ができず、GERDによる生命を脅かす合併症(心肺機能不全など)がある場合
- 最適な治療に抵抗性の症状がある場合
- GERD関連の合併症のリスクが高い慢性疾患(神経障害、嚢胞性線維症など)がある場合
- GERDの徴候や症状をコントロールするために慢性的な薬物療法が必要である場合
考察と感想
逆流防止手術に関してでした。日本とは異なるプラクティスになるため、解釈が難しいですね。大まかな点としては、予防的に行うのではなく、症例ずつ個別にきちんと検討しましょうというところでしょうか。
日米での違いを理解するには、それぞれの文献を読む必要がありそうですね。
参考文献も読んでみようと思います:
Goldin AB, Garrison M, Christakis D. Variations between hospitals in antireflux procedures in children. Archives of Pediatrics & Adolescent Medicine. 2009;163(7):658-663.
Rosen R, Vandenplas Y, et al. Pediatric Gastroesophageal Reflux Clinical Practice Guidelines: Joint Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition (NASPGHAN) and the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN). Journal of Pediatric Gastroenterology and Nutrition. 2018. March 66(3):516-554
Albanese CT, Towbin RB, et al.. Percutaneous gastrojejunostomy versus Nissen fundoplication for enteral feeding of the neurologically impaired child with gastroesophageal reflux. The Journal of Pediatrics. 1993;123(3):371-375.
Fonkalsrud EW, Ashcraft KW, et al. Surgical treatment of gastroesophageal reflux in children: a combined hospital study of 7467 patients. Pediatrics. 1998;101(3 Pt 1):419-422.
Smith CD, Othersen HB, Jr., et al. Nissen fundoplication in children with profound neurologic disability. High risks and unmet goals. Annals of Surgery. 1992;215(6):654-658; discussion 658-659.
Barnhart DC, Hall M, et al. Effectiveness of fundoplication at the time of gastrostomy in infants with neurological impairment. JAMA Pediatrics. 2013;167(10):911-918.
Jancelewicz T, Lopez ME, et al. Surgical management of gastroesophageal reflux disease (GERD) in children: A systematic review. Journal of Pediatric Surgery. 2017;52(8):1228-1238.
まとめ
今回は、小児の胃瘻挿入時に逆流防止手術に関するchoosing wiselyをご紹介しました。
これ以外にも項目が出ているようなので、コツコツと読んでいこうと思います。

Dr. KIDの執筆した書籍・Note
医学書:小児のかぜ薬のエビデンス
小児のかぜ薬のエビデンスについて、システマティックレビューとメタ解析の結果を中心に解説しています。
また、これらの文献の読み方・考え方についても「Lecture」として解説しました。
1冊で2度美味しい本です:

小児の診療に関わる医療者に広く読んでいただければと思います。
医学書:小児の抗菌薬のエビデンス
こちらは、私が3年間かかわってきた小児の抗菌薬の適正使用を行なった研究から生まれた書籍です。
日本の小児において、現在の抗菌薬の使用状況の何が問題で、どのようなエビデンスを知れば、実際の診療に変化をもたらせるのかを、小児感染症のエキスパートの先生と一緒に議論しながら生まれた書籍です。

noteもやっています
当ブログの注意点について
当ブログは医療関係者・保護者の方々に、科学的根拠に基づいた医療情報をお届けするのをメインに行なっています。参考にする、勉強会の題材にするなど、個人的な利用や、閉ざされた環境で使用される分には構いません。
一方で、当ブログ記事を題材にして、運営者は寄稿を行なったり書籍の執筆をしています。このため運営者の許可なく、ブログ記事の盗用、剽窃、不適切な引用をしてメディア向けの資料(動画を含む)として使用したり、寄稿をしないようお願いします。
ブログの記載やアイデアを公的に利用されたい場合、お問い合わせ欄から運営者への連絡お願いします。ご協力よろしくお願いします。