Stage 3-5のCKDにおいて、小児の腎臓内科専門医への相談なしにCVやPICCを留置しない[choosing wisely]
今回は、CKDのある小児のCVやPICCに関してです。
この推奨を「choosing wisely」ではどのように記載されているのか紹介してみようと思います。

- Choosing wisely:CKDのある小児のCVやPICCに関して
- 小児の腎臓内科専門医への相談なしにCVやPICCを留置しない
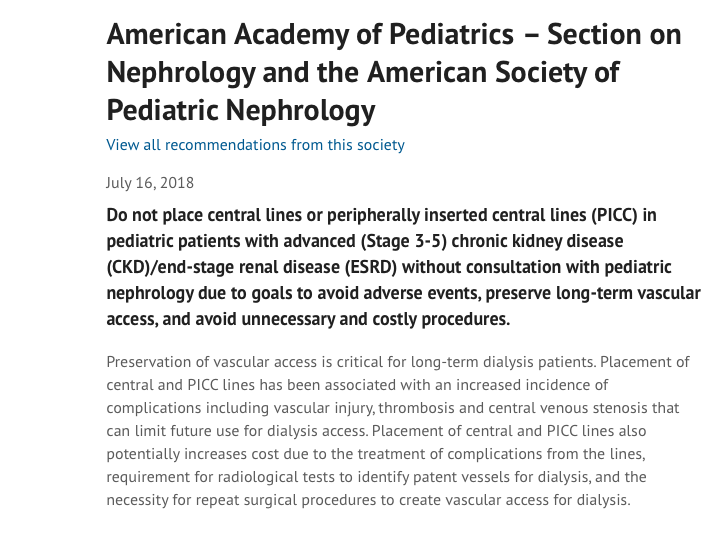
American Academy of PediatricsからのChoosing Wisely
Stage 3-5のCKDにおいて、小児の腎臓内科専門医への相談なしにCVやPICCを留置しない[Choosing wisely]
Do not place central lines or peripherally inserted central lines (PICC) in pediatric patients with advanced (Stage 3-5) chronic kidney disease (CKD)/end-stage renal disease (ESRD) without consultation with pediatric nephrology due to goals to avoid adverse events, preserve long-term vascular access, and avoid unnecessary and costly procedures.
Preservation of vascular access is critical for long-term dialysis patients. Placement of central and PICC lines has been associated with an increased incidence of complications including vascular injury, thrombosis and central venous stenosis that can limit future use for dialysis access. Placement of central and PICC lines also potentially increases cost due to the treatment of complications from the lines, requirement for radiological tests to identify patent vessels for dialysis, and the necessity for repeat surgical procedures to create vascular access for dialysis.
Studies in children are limited, but research about PICC lines demonstrates a 23-57 percent incidence of thrombosis in adults and increased complications in children who are exposed to multiple PICC line placements. Studies from adult patients have demonstrated the high risk of vascular injury after central line and PICC line placement. National guidelines from the Kidney Disease Outcomes Quality Initiative (KDOQI) have recommended avoiding placement of central lines in CKD patients, if possible, due to the high risk of complications. The recommendation to avoid central line placement is the basis of vascular access preservation in the “Fistula First Innovation” program for adult dialysis patients. National guidelines from the Kidney Disease Outcomes Quality Initiative (KDOQI) state the following: “In patients with CKD stage 4 or 5, forearm and upper-arm veins suitable for placement of vascular access should not be used for venipuncture or for the placement of intravenous (IV) catheters, subclavian catheters, or peripherally inserted central catheter lines (PICCs). Because of the substantial risk for loss of useable upper-extremity veins and central venous stenosis with PICCs, the Work Group recommends strongly that PICCs not be used in patients with CKD”. Special consideration may be necessary in emergency circumstances in which no other safe access is achievable.
進行期(ステージ3~5)の慢性腎臓病(CKD)/末期腎不全(ESRD)の小児患者において、有害事象の回避、長期的なバスキュラーアクセスの確保、不必要でコストのかかる処置の回避を目的として、小児腎臓内科専門医との相談なしに中心静脈カテーテル(CVC)や末梢挿入型セントラルライン(PICC)を留置してはいけません。
長期透析患者にとって、バスキュラーアクセスを確保することは非常に重要です。
中心静脈やPICCラインを留置すると、血管損傷、血栓症、中心静脈狭窄などの合併症の発生率が高くなり、将来的に透析アクセスに使用できなくなる可能性があります。
また、CVCやPICCラインの留置は、合併症の治療、透析用の血管を確保するための放射線検査、透析用の血管を確保するための外科手術の繰り返しなどにより、費用が増加する可能性があります。
小児を対象とした研究は限られていますが、PICCラインに関する研究では、成人では血栓症の発生率が23~57%であり、PICCラインを何度も留置する小児では合併症が増加することが示されています。
成人患者を対象とした研究では、CVCやPICC留置後の血管損傷のリスクが高いことが示されています。
Kidney Disease Outcomes Quality Initiative(KDOQI)の全国ガイドラインでは、合併症のリスクが高いため、CKD患者には可能な限りセントラルラインの留置を避けることが推奨されている。
成人透析患者を対象とした “Fistula First Innovation “プログラムでは、CVCの留置を避けるという推奨がバスキュラーアクセス保全の基本となっています。
Kidney Disease Outcomes Quality Initiative(KDOQI)の全米ガイドラインでは、以下のように述べられています:「CKDステージ4または5の患者では、バスキュラーアクセスの設置に適した前腕および上腕の静脈は、静脈穿刺、静脈内カテーテル、鎖骨下カテーテル、または末梢挿入型中心カテーテルライン(PICC)の設置に使用してはならない。PICCを使用すると、使用可能な上肢静脈が失われたり、中心静脈が狭窄したりする大きなリスクがあるため、作業部会ではCKD患者にPICCを使用しないことを強く推奨しています」。
他に安全なアクセスができない緊急事態には、特別な配慮が必要かもしれません。
考察と感想
CKDのある小児のCVやPICCに関してでした。小児のchoosing wiselyを沢山読んできましたが、その中でも最長の文章で下値。
参考文献も読んでみようと思います:
Yang RY, Moineddin R, Filipescu D, Parra D, Amaral J, John P, Temple M, Connolly B: Increased complexity and complications associated with multiple peripherally inserted central catheter insertions in children: the tip of the iceberg. J Vasc Interv Radiol 23:351-357, 2012.
Costello JM, Clapper TC, Wypij D. Minimizing complications associated with percutaneous central venous catheter placement in children: recent advances. Pediatr Crit Care Med 2013; 14:273–283.
KDOQI Vascular access guidelines 2006 Volume 48, Supplement 1, Pages S176–S247.
McGill R, Ruthazer R, Meyer K, Miskulin D, Weiner D: Peripherally Inserted Central Catheters and Hemodialysis Outcomes. Clin J Amer Soc Nephrol 11:1434-1440, 2016.
Gonzalves CF, et al: Incidence of central venous stenosis and occlusion following upper extremity PICC and port placement. Cardiovasc Intervent Radiol 26:123-127, 2003.
Forauer AR, Theoharis C: Histologic changes in the human vein wall adjacent to indwelling central venous catheters. J Vasc Interv Radiol 14:1163-1168, 2003.
まとめ
今回は、CKDのある小児のCVやPICCに関するchoosing wiselyをご紹介しました。
これ以外にも項目が出ているようなので、コツコツと読んでいこうと思います。

Dr. KIDの執筆した書籍・Note
医学書:小児のかぜ薬のエビデンス
小児のかぜ薬のエビデンスについて、システマティックレビューとメタ解析の結果を中心に解説しています。
また、これらの文献の読み方・考え方についても「Lecture」として解説しました。
1冊で2度美味しい本です:

小児の診療に関わる医療者に広く読んでいただければと思います。
医学書:小児の抗菌薬のエビデンス
こちらは、私が3年間かかわってきた小児の抗菌薬の適正使用を行なった研究から生まれた書籍です。
日本の小児において、現在の抗菌薬の使用状況の何が問題で、どのようなエビデンスを知れば、実際の診療に変化をもたらせるのかを、小児感染症のエキスパートの先生と一緒に議論しながら生まれた書籍です。

noteもやっています
当ブログの注意点について
当ブログは医療関係者・保護者の方々に、科学的根拠に基づいた医療情報をお届けするのをメインに行なっています。参考にする、勉強会の題材にするなど、個人的な利用や、閉ざされた環境で使用される分には構いません。
一方で、当ブログ記事を題材にして、運営者は寄稿を行なったり書籍の執筆をしています。このため運営者の許可なく、ブログ記事の盗用、剽窃、不適切な引用をしてメディア向けの資料(動画を含む)として使用したり、寄稿をしないようお願いします。
ブログの記載やアイデアを公的に利用されたい場合、お問い合わせ欄から運営者への連絡お願いします。ご協力よろしくお願いします。