早産児における気管支肺異形成の予防または治療を目的に、高用量デキサメタゾンを使用しない[Choosing wisely]
今回は、早産児における気管支肺異形成の予防または治療を目的とした高用量のデキサメタゾンに関してです。
この推奨を「choosing wisely」ではどのように記載されているのか紹介してみようと思います。

- Choosing wisely:BPDの予防としてのステロイドに関して
- 高用量のデキサメタゾン(0.5mg/kg/日)を使用しない
- 低用量に関しては有効性を示唆した研究がある
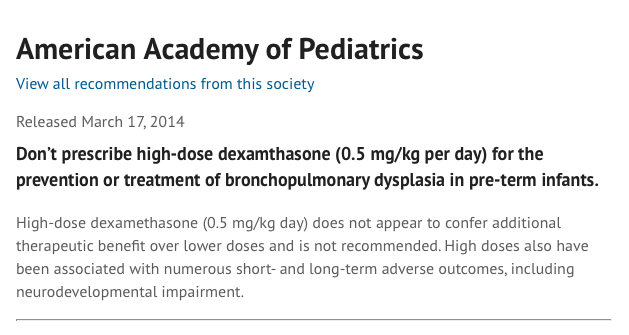
Don’t prescribe high-dose dexamthasone for the prevention or treatment of bronchopulmonary dysplasia in pre-term infants.
American Academy of PediatricsからのChoosing Wisely
早産児における気管支肺異形成の予防または治療を目的に、高用量デキサメタゾンを使用しない[Choosing wisely]
Don’t prescribe high-dose dexamthasone (0.5 mg/kg per day) for the prevention or treatment of bronchopulmonary dysplasia in pre-term infants.
High-dose dexamethasone (0.5 mg/kg day) does not appear to confer additional therapeutic benefit over lower doses and is not recommended. High doses also have been associated with numerous short- and long-term adverse outcomes, including neurodevelopmental impairment.
早産児における気管支肺異形成の予防または治療を目的に、高用量のデキサメタゾン(0.5mg/kg/日)を使用しない。
高用量デキサメタゾン(0.5mg/kg/日)は、低用量よりも追加的な治療上の有益性を与えるようには見えず、推奨されない。
高用量はまた、神経発達障害を含む多数の短期および長期の有害転帰と関連している。
考察と感想
早産児における気管支肺異形成におけるステロイドの意義について解説されたものでした。
2010年のPediatrics誌の記載をもとに書かれているようですね。

BPD remains a major morbidity of the extremely preterm infant and is consistently associated with adverse effects on long-term outcomes, including neurodevelopment. Additional RCTs of postnatal glucocorticoids are warranted to optimize therapy and improve outcomes for these infants. Those who design such trials in the future should attempt to minimize the use of open-label glucocorticoid, which has confounded analysis of most previous trials, and should include assessment of long-term pulmonary and neurodevelopmental outcomes.
High daily doses of dexamethasone (approximately 0.5 mg/kg per day) have been shown to reduce the incidence of BPD but have been associated with numerous short- and long-term adverse outcomes, including neurodevelopmental impairment, and at present there is no basis for postulating that high daily doses confer additional therapeutic benefit over lower-dose therapy. Recommendation: in the absence of randomized trial results showing improved short- and long-term outcomes, therapy with high-dose dexamethasone cannot be recommended.
Low-dose dexamethasone therapy (<0.2 mg/kg per day) may facilitate extubation and may decrease the incidence of short- and long-term adverse effects observed with higher doses of dexamethasone. Additional RCTs sufficiently powered to evaluate the effects of low-dose dexamethasone therapy on rates of survival without BPD, as well as on other short- and long-term outcomes, are warranted. Recommendation: there is insufficient evidence to make a recommendation regarding treatment with low-dose dexamethasone.
Low-dose hydrocortisone therapy (1 mg/kg per day) given for the first 2 weeks of life may increase rates of survival without BPD, particularly for infants delivered in a setting of prenatal inflammation, without adversely affecting neurodevelopmental outcomes. Clinicians should be aware of a possible increased risk of isolated intestinal perforation associated with early concomitant treatment with inhibitors of prostaglandin synthesis. Further RCTs powered to detect effects on neurodevelopmental outcomes, aimed at targeting patients who may derive most benefit and developing treatment strategies to reduce the incidence of isolated intestinal perforation, are warranted. Recommendation: early hydrocortisone treatment may be beneficial in a specific population of patients; however, there is insufficient evidence to recommend its use for all infants at risk of BPD.
Higher doses of hydrocortisone (3–6 mg/kg per day) instituted after the first week of postnatal age have not been shown to improve rates of survival without BPD in any RCT. RCTs powered to assess the effect of this therapy on short- and long-term outcomes are needed. Recommendation: existing data are insufficient to make a recommendation regarding treatment with high-dose hydrocortisone.
低用量のステロイドに関しては有効性を示唆する研究はあるものの、低用量ではなく高用量にするメリットを推奨できるような研究結果は不十分といったところでしょうか。
まとめ
今回は、J早産児における気管支肺異形成におけるステロイドに関するchoosing wiselyをご紹介しました。
これ以外にも項目が出ているようなので、コツコツと読んでいこうと思います。

Dr. KIDの執筆した書籍・Note
医学書:小児のかぜ薬のエビデンス
小児のかぜ薬のエビデンスについて、システマティックレビューとメタ解析の結果を中心に解説しています。
また、これらの文献の読み方・考え方についても「Lecture」として解説しました。
1冊で2度美味しい本です:

小児の診療に関わる医療者に広く読んでいただければと思います。
医学書:小児の抗菌薬のエビデンス
こちらは、私が3年間かかわってきた小児の抗菌薬の適正使用を行なった研究から生まれた書籍です。
日本の小児において、現在の抗菌薬の使用状況の何が問題で、どのようなエビデンスを知れば、実際の診療に変化をもたらせるのかを、小児感染症のエキスパートの先生と一緒に議論しながら生まれた書籍です。

noteもやっています
当ブログの注意点について
当ブログは医療関係者・保護者の方々に、科学的根拠に基づいた医療情報をお届けするのをメインに行なっています。参考にする、勉強会の題材にするなど、個人的な利用や、閉ざされた環境で使用される分には構いません。
一方で、当ブログ記事を題材にして、運営者は寄稿を行なったり書籍の執筆をしています。このため運営者の許可なく、ブログ記事の盗用、剽窃、不適切な引用をしてメディア向けの資料(動画を含む)として使用したり、寄稿をしないようお願いします。
ブログの記載やアイデアを公的に利用されたい場合、お問い合わせ欄から運営者への連絡お願いします。ご協力よろしくお願いします。